
Let’s Talk!
We’re here to help you with any questions you may have. Please don’t hesitate to reach out to us.
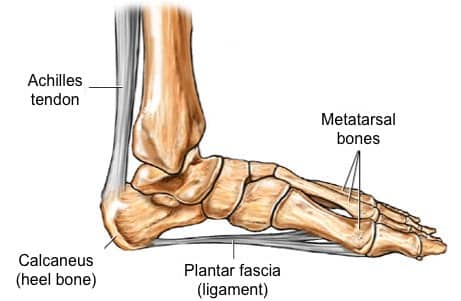

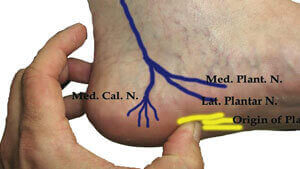
Plantar fasciitis is the most frequently reported and disabling disorder of the foot, but very little is known about the exact cause. It is thought that ongoing injury which causes microtearing and persistent inflammation of the plantar fascia at its origin (i.e. calcaneus) resulting in the degeneration of the connective tissue band(9).
It has been suggested that plantar fasciitis represents a form of tennis elbow at the heel with the condition being caused by repetitive microtrauma at the point of insertion of the plantar fascia.
Whenever the heel is in contact with the ground (such as during walking), the foot automatically pronates due to inward movement of tibia. This leads to stretching of the plantar fascia and the pressure generated due to this stretching flattens the plantar arches. In simple words, this arrangement acts like shock absorbers in accommodating the pressure and stress from walking. In the presence of certain contributing risk factors (listed above such as obesity, improper foot gear etc.), the fibers of plantar fascia undergo excessive stretching and micro tearing(1)(10). Most commonly, the micro-tearing begins at the site of origin of Plantar Fasciitis – the medial prominence or tuberosity of the calcaneus. If left untreated, the process of tearing causes degeneration of fascial fibers and associated connective tissue elements.
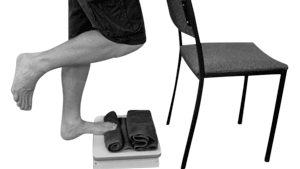
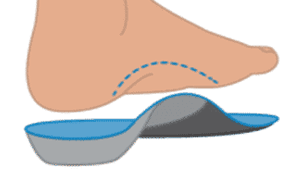
 Plantar fasciitis is usually a self-resolving condition especially when treated early with conservative treatments. However, once the degeneration and persistent inflammatory reaction sets in, it is usually a downhill course. The plantar fasciitis usually presents with persistent pain in the infero-medial aspect of the heel. The pathophysiology of pain is complex and is often described as a multitude of various pathological processes such as loss of normal elasticity of fascial fibers, abnormal changes in the vascularity due to fibrosis, thickening of the plantar fascia and inflammatory destruction. In the absence of any meaningful interventions to control the process or minimize the ongoing damage (stretching, orthotics, shoes modification, night splinting etc.), most patients develop severe morbidity and disability.
Plantar fasciitis is usually a self-resolving condition especially when treated early with conservative treatments. However, once the degeneration and persistent inflammatory reaction sets in, it is usually a downhill course. The plantar fasciitis usually presents with persistent pain in the infero-medial aspect of the heel. The pathophysiology of pain is complex and is often described as a multitude of various pathological processes such as loss of normal elasticity of fascial fibers, abnormal changes in the vascularity due to fibrosis, thickening of the plantar fascia and inflammatory destruction. In the absence of any meaningful interventions to control the process or minimize the ongoing damage (stretching, orthotics, shoes modification, night splinting etc.), most patients develop severe morbidity and disability. 











We’re here to help you with any questions you may have. Please don’t hesitate to reach out to us.
