Heel spurs are quite common even in the general population and are usually not associated with any symptoms of discomfort or inflammation. The decisions regarding to surgical approach and remove heel spur is dependent on:
Heel spurs are quite common even in the general population and are usually not associated with any symptoms of discomfort or inflammation. The decisions regarding to surgical approach and remove heel spur is dependent on:
- Size of the heel spur
- Anatomical alignment or positioning of spur (backward facing or forward facing)
- Location of the heel spur
- Co-existing condition of the foot and severity/ nature of symptoms.

Several factors are considered while performing open plantar fasciotomy; such as incision placement, release of plantar fascia and post-release stabilization. Traditional open plantar release can be performed by multiple approaches.
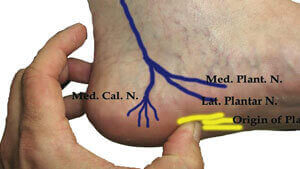
Plantar (bottom of the foot) incision is the most preferred approach in chronic cases as it gives maximum visualization of the plantar ligaments and associated structures such as heel spur.
If plantar fascia is thick and diseased, use of in-step plantar approach (a variant of traditional plantar approach) helps in facilitating selective release of the plantar fascia and speedy post-operative healing. In addition, this approach is also associated with minimal risk of adverse effects and long-term complications. However, immediate post-operative weight bearing should be avoided to allow maximal healing to plantar incision.

Endoscopic plantar fasciotomy (or endoscopic plantar fascia release) is a relatively new procedure that is associated with minimal surgical dissection of the tissue with the help of delicate instrumentation and precise tissue resection. The surgical resection of plantar fascia is always performed under direct visualization via endoscopic cameras.
The key features of endoscopic fasciotomy vs. an open approach are:
- Relatively faster rehabilitation period and overall shorter recovery period;
- Patients can expect early return to normal functioning; and,
- Immediate post-procedure weight- bearing
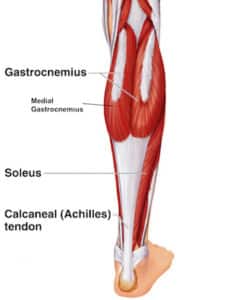
Depending upon the pathophysiology and other patient factors, other surgical procedures can also be attempted such as proximal medial gastrocnemius release (also referred to as PMGR). A fair chunk of plantar fasciitis patients have isolated rigidity or tightness of gastrocnemius muscle which significantly impairs the bio-mechanics of the lower limb (both knee and ankle joint); leading to limited ankle movement (coupled with altered knee extension). This surgical procedure is especially helpful in these patients to minimize the risk of recurrence of plantar fasciitis. Patient satisfaction scores are quite high with PMGR (more than 95%) and most patients are able to resume their normal day-to-day operations within 3 weeks after the procedure.