 If conservative measures are unsuccessful at eliminating plantar fasciitis pain, Extracorporeal Shock Wave Therapy (ESWT) is considered an excellent next step. We use a type of ESWT called Extracorporeal Pulse Activation Technology or EPAT®). We provide it as a simple and excellent treatment of plantar fasciitis. Recently, EPAT has also been shown to be very effective when used in early plantar fasciitis.
If conservative measures are unsuccessful at eliminating plantar fasciitis pain, Extracorporeal Shock Wave Therapy (ESWT) is considered an excellent next step. We use a type of ESWT called Extracorporeal Pulse Activation Technology or EPAT®). We provide it as a simple and excellent treatment of plantar fasciitis. Recently, EPAT has also been shown to be very effective when used in early plantar fasciitis.
Extracorporeal Pulse Activation Technology uses high frequency sound waves that are directed at the most tender part of the heel to promote healing. EPAT offers fast recovery without the necessity of reduced weight bearing or immobilization. The short recovery time allows the patients to resume their daily living activities earlier.
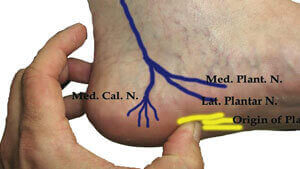
 Ultrasound guided radiofrequency ablation is a sophisticated, minimally invasive procedure for Plantar Fasciitis. High patient satisfaction scores and long-term pain relief have been reported, especially for patients whose Plantar Fasciitis pain is due to Baxter’s Entrapment. The accuracy and precision of the procedure is significantly improved with the use of ultrasound and nerve stimulator guidance.
Ultrasound guided radiofrequency ablation is a sophisticated, minimally invasive procedure for Plantar Fasciitis. High patient satisfaction scores and long-term pain relief have been reported, especially for patients whose Plantar Fasciitis pain is due to Baxter’s Entrapment. The accuracy and precision of the procedure is significantly improved with the use of ultrasound and nerve stimulator guidance.
Radiofrequency ablation uses high frequency sound waves to heat the affected sensory nerve to 90 degrees Celsius. At this temperature, proteins in the nerve are broken down and the nerve is destroyed, which prevents the nerve fibers from transmitting pain from that area. Radiofrequency ablation can also stimulate the creation of new blood vessels, which accelerates the healing process. At our center, the intervention is performed
 Platelet rich plasma (PRP) treatment is the injection of the patient’s own platelets to jumpstart the healing process for soft tissue injuries such as injured tendons, ligaments, muscles, joints and plantar fasciitis.
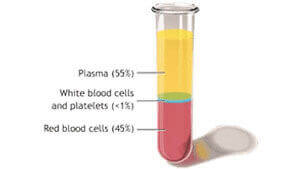
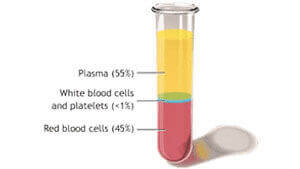
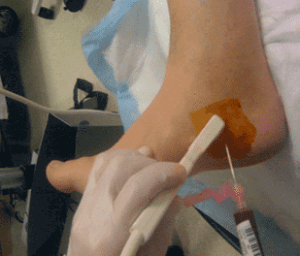
The use of platelet-rich plasma injections for plantar fasciitis is relatively new. Recent studies have shown platelet-rich plasma injections to be effective in treating plantar fasciitis. Some studies even suggest that these injections should be adopted as the first line of treatment especially with recently developed injection techniques. Platelet activation plays a key role in the process of wound and soft tissue healing, especially when inflammation is present. Platelet-rich plasma injections are prepared by centrifuging the patient’s own blood to create a high concentration of platelets, around 7-10 times the concentration found in regular blood. These concentrated activated platelets are injected into the abnormal tissue, causing a local inflammatory reaction which releases growth factors that stimulate healing , tissue regeneration and accelerate recovery. The activated platelets also
Platelet rich plasma (PRP) treatment is the injection of the patient’s own platelets to jumpstart the healing process for soft tissue injuries such as injured tendons, ligaments, muscles, joints and plantar fasciitis.
The use of platelet-rich plasma injections for plantar fasciitis is relatively new. Recent studies have shown platelet-rich plasma injections to be effective in treating plantar fasciitis. Some studies even suggest that these injections should be adopted as the first line of treatment especially with recently developed injection techniques. Platelet activation plays a key role in the process of wound and soft tissue healing, especially when inflammation is present. Platelet-rich plasma injections are prepared by centrifuging the patient’s own blood to create a high concentration of platelets, around 7-10 times the concentration found in regular blood. These concentrated activated platelets are injected into the abnormal tissue, causing a local inflammatory reaction which releases growth factors that stimulate healing , tissue regeneration and accelerate recovery. The activated platelets also  The use of ultrasound for the injection of platelet rich plasma increases the precision of injection and the quality of results while decreasing the likelihood of complications. PRP injection therapy is generally completed in just one session, but may require additional injections depending upon the clinical circumstances.
The use of ultrasound for the injection of platelet rich plasma increases the precision of injection and the quality of results while decreasing the likelihood of complications. PRP injection therapy is generally completed in just one session, but may require additional injections depending upon the clinical circumstances.
Since the procedure involves utilization of the patient’s own blood, the risk of adverse effects or complications is low. The procedure is generally well tolerated with high patient satisfaction scores and long term pain relief. Some side effects of platelet rich plasma injections are post-injection swelling and localized discomfort that usually goes away in a couple of days. Ice or over-the-counter analgesics (like Acetaminophen (Tylenol) but not NSAIDs) can help reduce discomfort after the procedure. Other less common risks of Platelet Rich Plasma injections include; infection, localized bruising or changes in skin color. PRP is contraindicated in breastfeeding/ pregnant women, individuals with known history of coagulation or bleeding disorders and malignant lesions. NSAIDs such as ibuprofen cannot be used after Platelet Rich Plasma injections since they interfere with the effectiveness of the PRP treatment.